Editor’s Note: This is an updated version of a Q&A we published Jan. 30. Much has changed since then.
 An outbreak of viral pneumonia that began in the central Chinese city of Wuhan at the end of 2019 has sickened more than 200,000 people and led to more than 8,000 deaths worldwide, as of March 18. (See the latest figures here.)
An outbreak of viral pneumonia that began in the central Chinese city of Wuhan at the end of 2019 has sickened more than 200,000 people and led to more than 8,000 deaths worldwide, as of March 18. (See the latest figures here.)
Scientists have made rapid progress in understanding the culprit, a new virus in the coronavirus family, which has been named severe acute respiratory syndrome coronavirus 2, or SARS-CoV-2. The pneumonia-like disease it causes is called COVID-19.
As the virus has spread, however, misinformation has, too. We’ve written about many bogus claims about the new coronavirus spread through social media, as well as false and misleading claims made by politicians. See our Coronavirus Coverage page for a guide to our articles.
Here, we answer some key questions about what is known so far about the outbreak and the virus.
When did the outbreak begin, and what is the cause?
Scientists are still working to determine when the virus first emerged in people, but the earliest known instances of the disease occurred in early December in Wuhan, a city of 11 million in central China.
After a string of mysterious pneumonia cases, many of them linked to a seafood market selling wild game and live animals, officials reported the outbreak to the World Health Organization on Dec. 31.
By Jan. 7, Chinese authorities had isolated a virus, later named SARS-CoV-2, as the cause of the disease, and shared the genome a few days later. This allowed other countries to test for the virus, and for scientists to begin devising treatments and investigating how the outbreak began.
Coronaviruses are a diverse family of large RNA viruses that have characteristic spikes on their surface, making them look like they have a halo, or corona, when viewed under a microscope.
Most coronaviruses that infect humans are relatively benign and cause mild respiratory diseases such as the common cold, said Susan Weiss, a coronavirus researcher at the University of Pennsylvania, in a phone interview.
But in recent years, new coronaviruses have cropped up that are far more dangerous to humans, including the severe acute respiratory syndrome, or SARS, virus, which led to a global outbreak in 2003, and the Middle East Respiratory Syndrome, or MERS, virus, which was identified in 2012.
According to the WHO, SARS ultimately infected more than 8,000 people, killing 774. Since 2012, there have been nearly 2,500 MERS cases and 858 deaths.
The new virus is fairly similar to the SARS virus — and is in the same betacoronavirus subgroup as both the SARS and MERS viruses — but is considered a new pathogen.
What are the symptoms, and how severe is the disease?
The virus causes a pneumonia-like respiratory illness that varies in severity, but can be deadly. Symptoms include fever, cough and shortness of breath.
A report in the Lancet that analyzed the first 41 people admitted to the hospital for COVID-19 infection suggests that clinically, the illness is similar to SARS, although fewer patients appear to have diarrhea or upper respiratory symptoms, such as sneezing, a runny nose and sore throat.
Some people also report fatigue, and in some cases people have been found to be infected, but clear of any symptoms.
Many of the symptoms are common to other respiratory diseases. Lab tests based on the virus’ genetic sequence can confirm infection.
It’s not yet known how frequently people die from COVID-19. The reported fatality rates have fluctuated as the disease has spread, hovering around 2-3% in late January, and around 4% as of March 18. For comparison, SARS killed around 10% of infected people, if not more, while seasonal influenza typically kills 0.1% or less, David Fisman, an epidemiologist at the University of Toronto, said in an email.
But these estimates, which are simple calculations of the number of deaths relative to the number of known cases, may not accurately reflect how dangerous the virus is, since the disease course is still underway for many patients, Fisman said. It’s also likely that far more people have been infected, but have not gone to hospitals or had their illnesses confirmed. For example, if two-thirds of cases are unreported, he said, the case fatality rate may be significantly lower. (For more on the fatality rate, see our March 5 story “Trump and the Coronavirus Death Rate.”)
According to a February study by the Chinese Center for Disease Control and Prevention, 14% of cases in mainland China were severe and 5% were critical.
Reports indicate that while healthy people can fall seriously ill and die, deaths are primarily in older folks and those with preexisting conditions such as diabetes, cardiovascular disease, chronic respiratory conditions and hypertension.
The Chinese CDC study, for instance, found a mortality rate of 14.8% in patients 80 and older and 8% for those 70 to 79, while the overall fatality rate then was 2.3% for cases in mainland China.
Similar statistics from Italy bear out this trend. As of March 15, no one in the country below the age of 30 had died from COVID-19, but a fifth or more of those above age 80 with the disease had. In Italy, about 25% of cases have been severe.
How is the virus transmitted, and how contagious is it?
The Centers for Disease Control and Prevention says the new coronavirus is transmitted from person to person in close contact, within about 6 feet of one another.
Scientists suspect the transmission is similar to how influenza is spread, with the virus travelling through respiratory droplets when infected people cough or sneeze. This is how scientists believe past coronaviruses such as SARS and MERS have spread.
The incubation period, or how long before someone who is infected shows symptoms, is estimated to be around 4 days, but may range from 2 to 14 days, according to the CDC. There is some evidence that asymptomatic people can transmit the virus to others. A March 16 Science study that modeled how the outbreak unfolded in China also found that people who have few or no symptoms may be responsible for the bulk of the disease spread. The CDC, however, says that people are “thought to be most contagious when they are most symptomatic” and that asymptomatic people are “not thought to be the main way the virus spreads.”
It also could be possible to contract the disease by touching a contaminated surface and then touching your mouth, nose or even eyes. A study released in mid-March by scientists with the National Institutes of Health, CDC, UCLA and Princeton found the virus could be detected for up to 24 hours on cardboard and much longer on hard surfaces including plastic and stainless steel — for up to two to three days.
At a March 18 press conference, coronavirus task force coordinator Dr. Deborah Birx said that “we’re still working out how much is it by human-human transmission and how much is it by surface,” adding that the fundamental guidelines are to avoid exposure to “excess number of persons who could be asymptomatic and infected … and don’t expose yourself to surfaces that could have had the virus on it.”
It’s also unclear exactly how infectious the new virus is. Several groups of scientists have attempted to estimate SARS-CoV-2’s basic reproduction number, or R0, which is the average number of other people one person infects, assuming everyone in the population is susceptible.
Using a variety of methods, multiple teams have arrived at figures that generally range from 1.5 to 4, which suggest the transmissibility is roughly in line with that of SARS, but below that of the measles virus, which has an R0 of around 12 to 18, and is one of the most infectious viruses in the world.
“Despite the diversity of approaches taken there’s remarkable consistency in estimates from highly competent investigators, which seem to fall between 2 and 3,” said Fisman.
An early estimate from the WHO, for example, suggested that every infected person would spread the virus to 1.4 to 2.5 people, on average, while a team at Imperial College London pegged the R0 at 2.6. A group at the University of Bern in Switzerland calculated an R0 of 1.4 to 3.8, and Harvard researchers Maia Majumder and Kenneth Mandl estimated a figure between 2 and 3.1.
While the figures provide some clue as to how contagious the virus is, it’s important to recognize that these values don’t necessarily say anything about how widespread the outbreak will be.
As Majumder pointed out on Twitter, the R0 reflects potential transmission, not actual transmission — and that even though seasonal flu has a relatively low R0 of about 1.3, it causes millions of cases per year, whereas SARS had an R0 between 2 and 5, and led to fewer than 10,000 cases.
“Planning, preparedness, and infection control can effectively bring an outbreak of a novel, moderate-R_0 disease to a close even in the absence of vaccines,” Majumder said in a tweet. “Because of this, estimates of R_0 for #nCoV2019 should be viewed as a call to action instead of a reason to panic.”
How can people protect themselves from contracting or spreading the virus?
The CDC advises people to wash their hands frequently, with soap and water for a minimum of 20 seconds, avoid touching their faces with unwashed hands, avoid close contact with sick individuals, and avoid social interactions generally to prevent community spread.
The CDC website provides advice on what to do if you’re sick and other resources.
Where have cases been reported?
On March 16, the WHO reported that the total cases and deaths outside China had surpassed those in China.
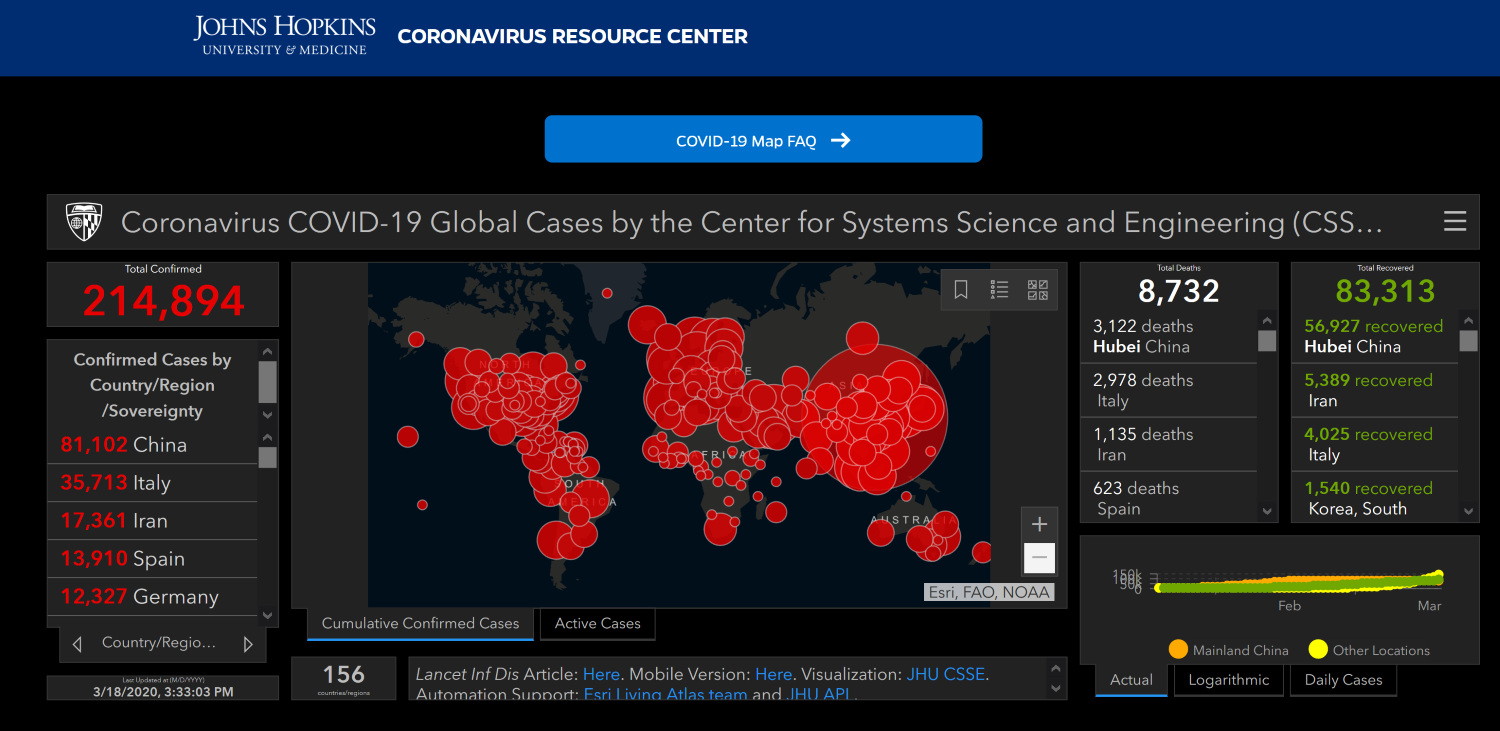
As of March 18, there have been 214,894 confirmed cases in 156 countries, from Greenland to the Caribbean nation St. Vincent and the Grenadines to the Maldives. The largest number of those cases — 81,102 — occurred in China.
{kind=link}
The second-largest total has been in Italy, with 35,713 cases, followed by Iran (17,361), Spain (13,910), Germany (12,327), France (9,052), South Korea (8,413), and the United States (7,769).
As of March 18, 8,732 people had died from COVID-19 worldwide.
Given the speed of the outbreak, these tallies will be out of date soon after we publish this article. Updates are available on a visualization tool put together by Johns Hopkins University.
The CDC also has launched its own state and global maps to show the location of the confirmed cases.
What information do we have about the U.S. cases?
The CDC announced the first American case on Jan. 21 in a man in his 30s who returned home to Washington state after a trip to Wuhan and then fell ill. Many more cases have followed, and the spread of the epidemic has accelerated.
As of March 18, there had been 7,769 cases confirmed in the U.S. But the total number of cases is thought to be quite a bit higher, given the fact that many patients have mild or possibly no symptoms and the U.S. has been slow to implement testing for COVID-19.
Cases of COVID-19 have been reported in all 50 states as well as the District of Columbia and the territories of Puerto Rico, Guam and the Virgin Islands. The states with the highest concentration of cases include Washington state, New York state and California.
As of March 18, there had been 118 fatal cases in the United States.
The Trump administration declared a public health emergency on Jan. 31, one day after the WHO did so, and announced a national emergency on March 13. Two days earlier, the WHO had declared the global outbreak a pandemic.
What are the U.S. travel restrictions?
The White House has issued a series of travel restrictions, beginning when Health and Human Services Secretary Alex Azar declared a public health emergency for the new coronavirus and announced travel restrictions to and from China, effective Feb. 2. That policy prohibits non-U.S. citizens, other than the immediate family of U.S. citizens and permanent residents, who have traveled to China within the last two weeks from entering the U.S. The special administrative regions of Hong Kong and Macau were excluded from the restrictions.
On Feb. 29, Trump expanded those travel restrictions to Iran. On March 11, those restrictions were extended to 26 European countries: Austria, Belgium, Czech Republic, Denmark, Estonia, Finland, France, Germany, Greece, Hungary, Iceland, Italy, Latvia, Liechtenstein, Lithuania, Luxembourg, Malta, Netherlands, Norway, Poland, Portugal, Slovakia, Slovenia, Spain, Sweden, and Switzerland. Three days later, on March 14, the president added the United Kingdom and Ireland to that list.
Although Trump has referred to the restrictions as a “travel ban” and said that he has “closed down the borders to China and to other areas that are very badly affected,” that’s not accurate. The restrictions exempt, for example, legal permanent residents of the U.S. and their immediate families, although there are travel warnings to many countries that Americans are asked to abide by. And although the president said on March 11 that European travel prohibitions would also pertain to a “tremendous amount of trade and cargo,” goods are not affected by the policy.
The U.S. temporarily closed its border with Canada to all non-essential traffic, Trump announced via Twitter on March 18.
For the latest information on travel restrictions by country, see the State Department’s page on COVID-19 Country Specific Information.
To date, there are no travel restrictions on domestic travel. In a press conference on March 16, Trump said, “We think that hopefully we won’t have to do that. But it’s certainly something that we talk about every day. We haven’t made that decision.”
The CDC has issued a list of things to consider when deciding whether it is safe to travel domestically, such as whether COVID-19 is spreading in the area where you are going and whether your travel would include “crowded settings, particularly closed-in settings with little air circulation” including conferences, public events or the use of public transportation.
For the latest travel information, visit the CDC’s COVID-19 Travel page, which includes information on international travel, cruise ship travel, health notices for each country and information for those returning from high-risk countries.
How is the rest of the world responding?
Measures taken by China have slowed the spread of new infections there, and some of the other countries that have been most affected are taking steps to prevent more cases within their own borders and abroad.
In Italy, which is second to China in the number of coronavirus cases and deaths, a nationwide lockdown went into effect on March 10. Residents can leave their homes for work, for health reasons and for basic needs, such as food shopping. Large gatherings in public spaces are prohibited, and restaurants and bars, which were first ordered to observe a 6 p.m. curfew, have been closed. Sporting events are cancelled, and schools, universities and recreational facilities are closed until at least April 3.
Spain recently announced a “state of alarm” and instituted a minimum 15-day lockdown similar to Italy’s, starting March 14. Politico Europe reported that “citizens can leave their homes only to buy groceries and pharmaceutical products, go to the bank or hospital, or to take care of dependents.” The newspaper added: “While on the street, they must be unaccompanied at all times, and while they can go to work, most workplaces are to be closed to the public until further notice.” The decree from Spain’s government also reportedly ordered the closing of “all schools, museums, libraries, hotels and restaurants, and prohibits sporting and cultural activities.”
Prior to that order, Spain had prohibited flights from Italy to Spain until March 25.
As of March 16, Germany reintroduced border checks at its land borders with Austria, Switzerland, France, Luxembourg and Denmark. Individuals with no valid reason for travel will not be permitted to enter or leave the country — particularly those with symptoms that could indicate they are infected with coronavirus. Also, schools and kindergartens in most German states have been closed until April 20, which is after the Easter holiday.
South Korea reportedly has had success reducing its rate of new infections because of its expansive testing program. As of March 17, South Korea had conducted nearly 287,000 tests for the coronavirus, according to the online publication Our World in Data. That was more than the next two countries, combined.
The South Korean government is also isolating infected individuals, as well as quarantining people with whom they have had contact, and using a tracking system to monitor their whereabouts to ensure they remain in the quarantine area.
Singapore also has been singled-out for its response to the outbreak. As of March 18, the nation of more than 5 million people had 313 confirmed cases of coronavirus and zero deaths, according to data from Johns Hopkins University.
In remarks in mid-February, WHO Director-General Tedros Adhanom Ghebreyesus said, “Singapore is leaving no stone unturned, testing every case of influenza-like illness and pneumonia.”
The island nation also made the decision early to “restrict entry for anyone from mainland China and, more recently, from northern Italy, Iran, and South Korea,” according to a March 6 article in The Lancet.
Reports also indicate that Singapore has made great efforts to track down people who have come in contact with infected people, and has strict rules for individuals in quarantine. Researchers in Singapore also were among the first to develop a test that can detect antibodies that remain in the body after someone has recovered from a coronavirus infection.
What information do we have on testing for COVID-19?
There were numerous problems initially that limited the availability of viral test kits and the number of people being tested in the U.S. We cover those in a March 10 story “The Facts on Coronavirus Testing.”
On March 3, Vice President Mike Pence announced that “any American can be tested with no restrictions, subject to doctor’s order.”
The CDC now recommends that those experiencing COVID-19 symptoms — including fever, cough and shortness of breath — call their doctor if they have been in “close contact” with someone who has tested positive for COVID-19 or are living in “a community where there is ongoing spread of COVID-19.”
Those at high risk, including the elderly and those with certain chronic medical conditions, should be tested “even if their illness is mild,” the CDC says.
Although testing is now available in all 50 states, the number of U.S. residents who have been tested remains relatively small.
As of March 17, the CDC said that CDC and public health laboratories have tested fewer than 32,000 samples. (The CDC provides daily updates on the number of samples that have been tested.) In addition, commercial labs have tested another 27,000 samples, bringing the total to 59,000, Adm. Brett Giroir, an assistant health secretary, said on March 17.
At a March 18 press conference, coronavirus task force coordinator Birx said the government is placing a priority on testing in “regions that were mostly affected. And so you still may have difficulty getting tests in areas that do not have significant cases.”
When will there be a COVID-19 vaccine and an antiviral treatment?
Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases, has said that a vaccine at best won’t be ready for “a year to a year-and-a-half” and won’t be available for the current epidemic.
“We can’t rely on a vaccine over the next several months to a year,” Fauci said at a Feb. 27 White House press conference. “However, if this virus, which we have every reason to believe it is quite conceivable that it will happen, will go beyond just a season and come back and recycle next year. If that’s the case, we hope to have a vaccine.”
On March 16, the National Institutes of Health announced that a Phase 1 clinical trial has begun at Kaiser Permanente Washington Health Research Institute in Seattle. The trial will involve 45 healthy adults ages 18 to 55 over a six-week period, NIH said.
But that is just the first phase of a lengthy process to make sure that the vaccine is effective and safe to use, as Fauci explained at a Feb. 25 press conference.
“[Y]ou need at least three to four months to determine if it’s safe and whether it induces the kind of response that you would predict will be protective,” Fauci said of the Phase 1 trial. “Once you do that you graduate to a much larger trial.”
A Phase 2 trial would involve “hundreds if not thousands of individuals to determine efficacy,” Fauci said. “That itself, even at rocket speed, would take at least an additional six to eight months. So when you are talking about the availability of a vaccine even to scale it up you’re talking about a year to a year-and-a-half.
As for an antiviral treatment, one could be ready by June at the earliest, officials say.
NIH announced on Feb. 25 that it had begun a “randomized, controlled clinical trial to evaluate the safety and efficacy of the investigational antiviral remdesivir in hospitalized adults diagnosed with coronavirus disease 2019 (COVID-19)” at the University of Nebraska.
“Remdesivir, developed by Gilead Sciences Inc., is an investigational broad-spectrum antiviral treatment,” NIH said in a press release. “It was previously tested in humans with Ebola virus disease and has shown promise in animal models for treating Middle East respiratory syndrome (MERS) and severe acute respiratory syndrome (SARS), which are caused by other coronaviruses.”
Daniel O’Day, chairman and CEO of Gilead Sciences, said at a March 2 White House meeting that the company hopes to know by April if the drug works. Fauci said “if the trial that Daniel is talking about proves efficacy, which you likely might know in a few months whether it’s … effective or not. If you know by June that it’s effective, then you just scale up and manufacture it, and you’re good to go.”
— by Jessica McDonald, Lori Robertson, Eugene Kiely, Robert Farley, Rem Rieder and D’Angelo Gore