SciCheck Digest
Rare cases of myocarditis have been reported following the mRNA COVID-19 vaccines, particularly among young males after a second dose. Most cases resolve quickly without the need for advanced therapies, although research on any potential long-term effects is ongoing. Nonetheless, the benefits of vaccination outweigh the risks in all populations, even in young males.
Full Story
Myocarditis, or inflammation of the heart muscle, is most often caused by a viral infection. Research shows that infection with SARS-CoV-2, the coronavirus that causes COVID-19, increases the risk of myocarditis across age groups. But myocarditis and pericarditis, inflammation of the outer lining of the heart, have also been identified as rare side effects of the mRNA COVID-19 vaccines.
![]() Most cases of vaccine-associated myocarditis have been observed in adolescents and young males ages 12 to 24, following a second dose. According to a Centers for Disease Control and Prevention study published in JAMA on Jan. 25, post-vaccine myocarditis is most frequent in the U.S. in males 16 to 17 years old, with 105.9 cases per million doses — or about 10.6 per 100,000.
Most cases of vaccine-associated myocarditis have been observed in adolescents and young males ages 12 to 24, following a second dose. According to a Centers for Disease Control and Prevention study published in JAMA on Jan. 25, post-vaccine myocarditis is most frequent in the U.S. in males 16 to 17 years old, with 105.9 cases per million doses — or about 10.6 per 100,000.
That study and others have found that compared with classic viral myocarditis, post-vaccine myocarditis appears to resolve faster and have better clinical outcomes, although investigations into potential long-term effects are ongoing. In patients with vaccine-associated myocarditis, symptoms such as chest pain, shortness of breath, palpitations or fatigue usually appear within a week of vaccination and resolve within a few days. Case studies show that most patients have been hospitalized, but most of them have recovered with rest and nonsteroidal anti-inflammatory drugs, such as ibuprofen, with very few needing intense therapies.
“In contrast, typical viral cases of myocarditis can have a more variable clinical course,” CDC experts point out in the JAMA study. “For example, up to 6% of typical viral myocarditis cases in adolescents require a heart transplant or result in mortality.”
Cardiologists interviewed for this story told us based on their experiences with patients, vaccine-associated myocarditis appears to be less frequent and severe than myocarditis following SARS-CoV-2 infection in adults, young adults and children. They said patients arriving to the hospital with heart inflammation after an infection often get admitted in the intensive care unit and need advanced therapies to rescue them, including an extracorporeal membrane oxygenation machine, a life support machine that takes over for a person’s heart and lungs.
“Post COVID-vaccination myocarditis, which has been shown to be less severe … typically does not require treatment and it runs its course. And does not require any other therapies other than just supportive care,” Dr. Joyce W. Wald, a cardiologist, medical director of the shock team and director of heart failure, transplant and mechanical circulatory support program at the University of Pennsylvania Health System, told us in an interview.
Dr. Matthew Elias, an attending cardiologist in the cardiac center at Children’s Hospital of Philadelphia, told us patients with heart issues triggered by COVID-19 go through a “very scary” and “life-threatening experience,” while those with myocarditis following vaccination are observed for a few days and their symptoms typically resolve with ibuprofen “or no medication at all, honestly.” “So very different experience room to room,” he said in a phone interview. Heart “issues are much more common, and they’re much more severe, with the infection compared to the vaccine.”
Preliminary CDC data on post-vaccine myocarditis in patients ages 12 to 29 show most patients had no impact on their quality of life and that 81% of them were either fully recovered or “probably fully recovered” and awaiting additional information, at least 90 days after a diagnosis.

Myocarditis and other complications associated with COVID-19, researchers and health officials emphasize, are more frequent than those linked to the vaccines, and the benefits of vaccination outweigh the risks in all populations, including male adolescents and young adults. A large study, published in Nature Medicine on Feb. 7, looked at cardiovascular outcomes in U.S. veterans one year after a SARS-CoV-2 infection and found that COVID-19 increased the risk for several heart disorders, including heart attacks, arrhythmias, strokes, cardiac arrests, and myocarditis.
SARS-CoV-2 infection can cause severe disease in children, too, either from COVID-19 or from a complication known as multisystem inflammatory syndrome in children. MIS-C is a rare syndrome following coronavirus infection in which at least two organs, often including the heart, become dangerously inflamed. The condition can cause myocarditis and may lead to acute heart failure in children.
Update, April 5: A CDC study published in the Morbidity and Mortality Weekly Report on April 1 found that the risk for cardiac complications including myocarditis, pericarditis and multisystem inflammatory syndrome was “significantly higher” after a SARS-CoV-2 infection than after receiving an mRNA COVID-19 vaccine, for both males and females in all age groups.
“Even among males aged 12–17 years, the group with the highest incidence of cardiac complications after receipt of a second mRNA COVID-19 vaccine dose, the risk was 1.8–5.6 times as high after SARS-CoV-2 infection than after vaccination,” the study says.
The incidence of myocarditis or pericarditis among males ages 12 to 17 was 56.0 to 64.9 cases per 100,000 after infection, compared with 26.7 to 35.9 after the second vaccine dose.
The study was based on 40 health care systems’ data on 15.2 million people ages 5 and up from Jan. 1, 2021, through Jan. 31, 2022.
No one in the U.S. is known to have died from vaccine-associated myocarditis, according to the CDC as of Jan. 13. In contrast, as of Feb. 23, there have been 5,796 COVID-19 deaths among people ages 18 to 29, and 851 COVID-19 deaths among those 17 and younger. Specifically in adolescents ages 16 to 17, where vaccine-associated myocarditis has occurred at the highest rate, there have been 1.8 million cases of COVID-19 reported and 327 COVID-19 related deaths, as of Feb. 24.
However, the rare risk of myocarditis continues to be misleadingly used to argue that COVID-19 vaccines are dangerous and that young males and children are better off without them.
There are plenty of examples of this in the media. We recently fact-checked a video of Dr. Robert Malone claiming, with no evidence, that COVID-19 vaccines “can damage your children” and that “many of these damages cannot be repaired.” We’ve also reported on unfounded claims that link COVID-19 vaccines to athletes collapsing or dying from myocarditis. Another example is Republican Sen. Rand Paul’s remarks in a Jan. 21 interview on Fox News’ “The Ingraham Angle.” In arguing that “it’s medical malpractice to force vaccines on children, particularly adolescent males,” he said: “We now have the scientific evidence that shows the risk of myocarditis for young males is greater for the vaccine than it is for the disease.”
Paul’s office told us his remarks were based on an unpublished paper posted to a preprint server on Dec. 25 by a team of researchers from the United Kingdom that found that in males under 40, the risk of myocarditis was higher following a second dose of the Moderna vaccine than after a SARS-CoV-2 infection. The preprint, nonetheless, concludes that for the overall population “the risk of hospital admission or death from myocarditis is greater following COVID-19 infection than following vaccination.” The same team had previously published a larger study in Nature Medicine with the same conclusion.
Paul’s remarks — as with most of the claims that use myocarditis to say that vaccines are dangerous for that age group — are missing context. As we have said, experts say the risk of myocarditis associated with the vaccine is rare and, more importantly, that everyone, including young males, could face much more serious outcomes from contracting COVID-19.
“COVID can kill you. COVID can cause you to go to the hospital, go to the intensive care unit, and die,” Dr. Paul Offit, director of the Vaccine Education Center at the Children’s Hospital of Philadelphia and a member of the FDA’s Vaccines and Related Biological Products Advisory Committee, told us in a phone interview. “Although I agree that the children are generally infected less frequently, and when they’re infected, they’re infected less severely — they can be infected severely, to the point that they are hospitalized or die.”
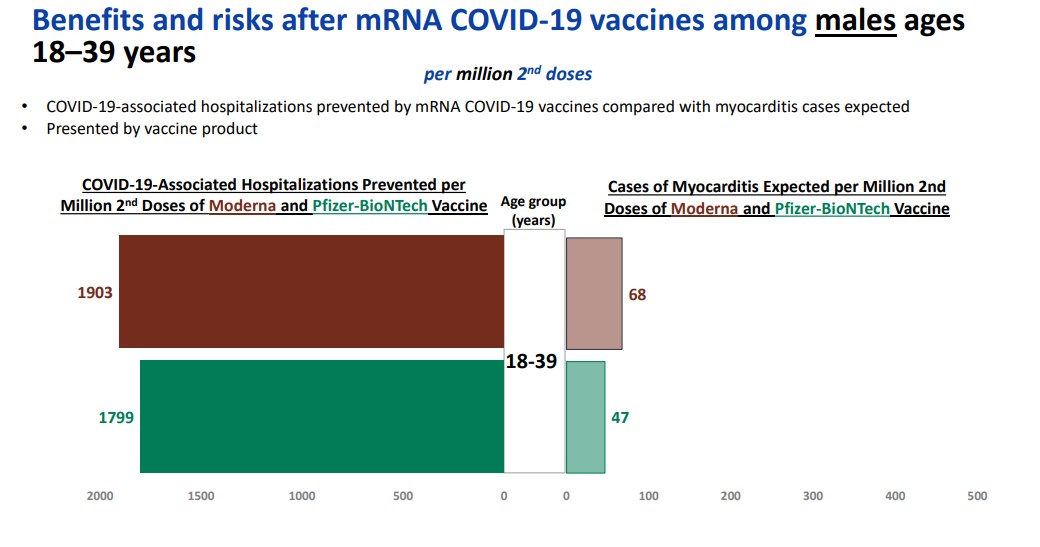
The CDC concluded as recently as Feb. 4 that the benefits of both mRNA COVID-19 vaccines “far outweigh” the risk of myocarditis, even in younger males. In a benefit-risk analysis presented to the agency’s Advisory Committee on Immunization Practices, the CDC estimated that for every million males between the ages of 18 and 39 who were vaccinated with a second dose, 1,799 and 1,900 hospitalizations would be avoided with the Moderna and Pfizer/BioNTech vaccines, respectively, compared with 68 and 47 expected cases of myocarditis per million second doses.
These estimates have inherent limitations. They are based on the agency’s current understanding of how often people are hospitalized with COVID-19 and develop vaccine-associated myocarditis, and they don’t reflect vaccine performance against omicron or factor in previous infection, for example. But even if they are off by a large margin, it’s likely the benefits would still outweigh the harms.
It’s nevertheless possible that if conditions change, such as if circulation of the coronavirus plummets, that the risk-benefit calculus could shift. In other words, if the risk of contracting COVID-19 is low, then fewer hospitalizations would be avoided through vaccination, reducing the benefit of vaccination for young males, potentially below the risk of vaccine-associated myocarditis.
But the current data strongly favor vaccination.
Myocarditis Following mRNA COVID-19 Vaccination
Evidence of an increased risk of myocarditis and pericarditis, particularly in young males and after a second dose of an mRNA vaccine, has been accumulating since it was first identified in May 2021. Experts say cases were not detected in clinical trials because the incidence in the general population was too small, with a rate of less than 4 per 100,000.
In June 2021, experts presented early data about the frequency of vaccine-associated myocarditis to the FDA’s Vaccines and Related Biological Products Advisory Committee and to the CDC’s Advisory Committee on Immunization Practices. CDC’s experts estimated the highest rate was 66.7 per million after a second dose among males ages 12 to 17, with the frequency declining in older males and generally lower rates in females. On June 23, the ACIP concluded that the benefits provided by the COVID-19 vaccines “clearly outweighed the risks of myocarditis after vaccination.” Fact sheets for patients and health care providers for the Moderna and Pfizer/BioNTech COVID-19 vaccines have included warnings since June 25.
Newer analyses have roughly confirmed those initial estimates.
According to the January CDC study published in JAMA, myocarditis remains a “rare but serious adverse event” of the mRNA COVID-19 vaccines. The analysis was based on 1,626 cases of myocarditis reported to the Vaccine Adverse Event Reporting System between December 2020 and August 2021, among 354,100, 845 doses of mRNA vaccines administered. It found that although the overall frequency of post-vaccine myocarditis is low, there was an increased risk of myocarditis for males and females across multiple age groups after vaccination. The highest rate of cases occurred after the second dose in adolescent males 16 to 17 years old (105.9 per million doses), followed by those 12 to 15 (70.7 per million doses), and those 18 to 24 years (52.4 per million doses of the Pfizer/BioNTech vaccine, and 56.3 per million doses of the Moderna vaccine).
Another recent study published in the New England Journal of Medicine on Jan. 26 by Israeli researchers found similar results. They tracked hospitalizations for myocarditis from June 2 to Oct. 20 among vaccinated adolescents ages 12 to 15 and found the rate of myocarditis cases in males was 0.56 per 100,000 after a first dose of the Pfizer/BioNTech vaccine, and 8.09 cases per 100,000 after the second (one case per 12,361.) The risk for female adolescents was much lower — 0.69 cases per 100,000 after the second dose. “All the cases were clinically mild,” Dr. Dror Mevorach, head of the Hadassah Hospital Ein Kerem’s internal medicine department, and his team reported in the study.
“The risks of myocarditis following second mRNA vaccination even in adolescent and young adult males remain low,” Dr. Leslie T. Cooper Jr., a myocarditis national expert and chair of the Department of Cardiology at the Mayo Clinic in Florida, told us in an email, “with most cases being mild. These risks should be weighed against the competing risks of hospitalization and death from infection” by the recent SARS-CoV-2 variants.
To explain what researchers mean by clinically mild, Wald, from Penn Medicine’s cardiology team, gave us some context. “Severe would be somebody coming in with myocarditis who’s unstable hemodynamically, meaning that they’re not getting enough blood, they’re in shock. … They need advanced therapies to rescue them from this event,” she said. Most patients with post-vaccine myocarditis do get hospitalized because “you’re going to want to make sure that you watch them and that it doesn’t turn into something more severe,” but the majority only need treatment with nonsteroidal anti-inflammatory drugs and were asymptomatic by the time they were discharged, she said. “So that’s what we mean by mild.”
The same applies to children. CHOP’s Elias says mild should be in quotes because kids with vaccine-associated myocarditis do typically get hospitalized and are observed for a few days. But it is referred to as mild because it’s “so much different” than MIS-C and also “much different and less severe” than classic myocarditis, he said.
“Children are typically admitted to the hospital, observed for a few days; they typically have normal heart function when we perform echocardiograms, and then, their symptoms, which is primarily chest pain, resolved quickly, within a day or two,” he said, “with minimal medication.”
The mechanisms for development of myocarditis after an mRNA COVID-19 vaccine are still not clear, although scientists have proposed a few possible mechanisms. Some experts believe sex hormones play a role. That would explain why it occurs mostly in younger males, similar to typical myocarditis.
“We don’t know the mechanism, but a theory that attributes a protective role to estrogen, or a risk associated with testosterone, is reasonable. It makes sense, at least based on epidemiological data,” Dr. Enrico Ammirati, a myocarditis expert at De Gasperis Cardio Center and Transplant Center at the Niguarda Hospital, in Italy, told Medscape Cardiology in January. He added, however, that scientists “do not have any direct evidence in human beings.”
Cooper told us some studies suggest that the risk of post-vaccine myocarditis is higher with the Moderna vaccine than with the Pfizer/BioNTech vaccine.
Some of the evidence presented on Feb. 4 at an ACIP meeting corroborates those findings. But after reviewing all the available data in a meeting that resulted in a recommendation for full approval of the Moderna vaccine for people 18 years and older, health officials said the “desirable consequences” of the vaccine still “clearly outweigh undesirable consequences in most settings.”
The FDA arrived at the same conclusion, according to documents presented when the vaccine was granted full approval on Jan. 31. According to the agency’s own benefit-risk assessment, based on the current evidence and a higher rate of post-vaccine myocarditis after a second dose in males ages 18 to 25, “the analyses support the benefits of vaccination over the risks of myocarditis/pericarditis for individuals ≥18 years of age.”
To mitigate the risk of myocarditis and improve vaccine effectiveness, several countries have recommended lengthening the interval between the mRNA vaccine doses from four weeks to between six and 12 weeks, while others recommended giving males or those under 30 the Pfizer/BioNTech vaccine. On Feb. 22, the CDC issued new COVID-19 mRNA vaccine guidance, recommending to extend the interval between the doses to eight weeks for “some people ages 12 and older, especially for males ages 12-39 years.”
“Some studies in adolescents (ages 12-17 years) and adults have shown the small risk of myocarditis associated with mRNA COVID-19 vaccines might be reduced and peak antibody responses and vaccine effectiveness may be increased with an interval longer than 4 weeks. Extending the interval beyond 8 weeks has not been shown to provide additional benefit. There are currently no data available for children ages 11 years and younger,” the CDC said.
Some countries paused or delayed second doses of mRNA vaccines in adolescents due to concerns of myocarditis, but then recommended them after the appearance of omicron. Taiwan, for example, stopped giving second doses for people ages 12 to 17 on Nov. 10, but resumed them by the end of the month. The U.K. delayed its recommendation for a second dose for adolescents ages 16 to 17 in August, but then went ahead with it in November.
In September, Hong Kong began advising that teens 12 to 17 years old receive only one dose of the Pfizer/BioNTech vaccine. A cohort study published in JAMA Pediatrics on Feb. 25 found the policy reduced the risk of myocarditis in that group. But as the authors explain, the study was conducted before omicron, when the country had virtually no local transmission of the virus and the risk of death or COVID-19 complications was “extremely low.” “In countries with large outbreaks and … prevalent local transmission, the risk-benefit assessment would favor a 2-dose regimen because the single-dose regimen provides suboptimal protection from severe outcomes associated with COVID-19,” the authors say.
In October, the FDA said it needed additional time to evaluate the emergency use authorization of the Moderna vaccine for adolescents 12 to 17 to analyze the risk of myocarditis after vaccination. No determination has been made to date.
Myocarditis Following SARS-CoV-2 Infection
As we previously said, COVID-19 and MIS-C, both caused by a SARS-CoV-2 infection, are associated with myocarditis.
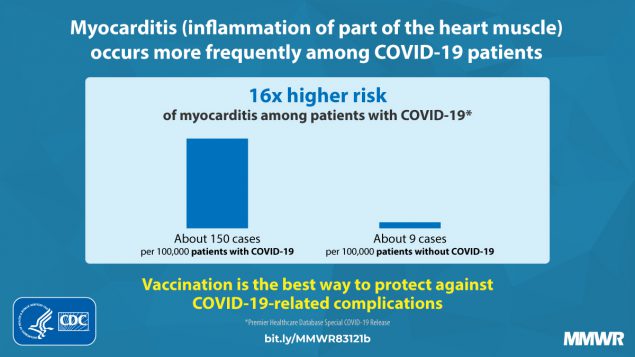
A CDC study, published in September 2021, found that patients with COVID-19 had nearly 16 times the risk for myocarditis than those without the disease, although the risk varied by sex and age. Male and female COVID-19 patients under 16 had almost 37 times the risk for myocarditis than those without infection, the study suggested. The risk was 7.4 times higher for patients between 16 and 24, and 6.7 times higher for patients 25 to 39 years old. Males had a higher risk than females.
About half of children with MIS-C, a rare complication of COVID-19 infection, develop myocarditis. As of Jan. 31, the CDC had reported 6,851 cases of multisystem inflammatory syndrome in children and 59 deaths, with most cases occurring in children 5 to 13.
Studies suggest that in the general population the risk of myocarditis is significantly higher after a SARS-CoV-2 infection than after vaccination.
A study from Israel published in the New England Journal of Medicine on Aug. 25, found that vaccination with the Pfizer/BioNTech vaccine was associated with a smaller excess risk of myocarditis (2.7 additional events per 100,000 people) than a SARS-CoV-2 infection (11 additional events per 100,000 people).
And a large study published in Nature Medicine that looked at rates of hospitalizations or death from myocarditis, pericarditis and cardiac arrhythmias following vaccination or a COVID-19 positive PCR test in the U.K. also found that infections were much more likely than vaccines to cause myocarditis and other heart complications.
“[W]hilst there are some increased risks of rare heart related complications associated with vaccines these are much lower than the risk associated with getting COVID-19. For example, we estimated between 1 and 10 extra events of myocarditis in 1 million people vaccinated with a first or second dose, but 40 extra cases in 1 million people infected with COVID-19,” Julia Hippisley-Cox, professor of clinical epidemiology and general practice at the University of Oxford and study lead, said in an interview for an Oxford website.
That study, though, did find differences in risk by age, with vaccine-associated myocarditis more likely among the under-40 crowd. “The risks are more evenly balanced in younger persons aged up to 40 years, where we estimated the excess in myocarditis events following SARS-CoV-2 infection to be 10 per million with the excess following a second dose of mRNA-1273 vaccine being 15 per million,” the authors wrote, referring to the Moderna vaccine.
The unpublished study that Paul cited to support his claim that “the risk of myocarditis for young males is greater for the vaccine than it is for the disease” is an expanded analysis by the same team, which added data from children ages 13 to 17 and from people receiving a booster. The new data didn’t change the conclusions for the overall population — “the risk of hospital admission or death from myocarditis is greater following COVID-19 infection than following vaccination,” it says. But it found that in males under 40, the risk of myocarditis following vaccination was “similar” to infection — and in what the authors termed a “notable exception,” the risk was higher than infection following a second dose of the Moderna vaccine in younger males.
It’s possible, then, that the risk of myocarditis is higher after a COVID-19 vaccine than after COVID-19 for certain people, particularly younger males. But that doesn’t mean people shouldn’t get vaccinated. Focusing solely on myocarditis is misleading because it ignores the fact that SARS-CoV-2 infection comes with other dangers, including a medley of other heart complications.
No vaccine or medical product is 100% safe, but as CHOP’s Offit told us, the choice to not get a vaccine is not a risk-free choice, either. “It’s just a choice to take a different risk,” he said. “And that different risk is the greater risk.”
Elias agrees. “Heart issues, whether we call it myocarditis or myocardial injury or MIS-C — these issues are much more common and they’re much more severe with the infection compared to the vaccine” in young people, he said. “I strongly recommend that everyone who’s eligible for the COVID-19 vaccine receive the vaccine as soon as possible.”
Editor’s note: SciCheck’s COVID-19/Vaccination Project is made possible by a grant from the Robert Wood Johnson Foundation. The foundation has no control over FactCheck.org’s editorial decisions, and the views expressed in our articles do not necessarily reflect the views of the foundation. The goal of the project is to increase exposure to accurate information about COVID-19 and vaccines, while decreasing the impact of misinformation.
Sources
National Institutes of Health, National Heart, Lung and Blood Institute. “Heart Inflammation.”
Cooper, Leslie T. “Myocarditis.” The New England Journal of Medicine. 09 Apr 2009.
Barda, Noam, et al. “Safety of the BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Setting.” The New England Journal of Medicine. 15 Aug 2021.
Kracalik, Ian. “Myocarditis Outcomes Following mRNA COVID-19 Vaccination.” Powerpoint presentation for Advisory Committee on Immunization Practices. 04 Feb 2022.
Boehmer, Tagan K., et al. “Association Between COVID-19 and Myocarditis Using Hospital-Based Administrative Data — United States, March 2020–January 2021.” Morbidity and Mortality Weekly Report. 03 Sep 2021.
Centers for Disease Control and Prevention. For Parents: Multisystem Inflammatory Syndrome in Children (MIS-C) associated with COVID-19. Updated 20 Sep 2021. Accessed 28 Feb 2022.
Centers for Disease Control and Prevention. Myocarditis and Pericarditis After mRNA COVID-19 Vaccination. Updated 12 Nov 2021. Accessed 28 Feb 2022.
Centers for Disease Control and Prevention. Weekly Updates by Select Demographic and Geographic Characteristics. Updated 23 Feb 2022. Accessed 28 Feb 2022.
Centers for Disease Control and Prevention. Demographic Trends of COVID-19 cases and deaths in the US reported to CDC. COVID Data tracker. Updated 27 Feb 2022.
Centers for Disease Control and Prevention. Safety of COVID-19 Vaccines. Updated 25 Feb 2022. Accessed 28 Feb 2022.
Centers for Disease Control and Prevention. Provisional COVID-19 Deaths: Focus on Ages 0-18 Years. Updated 02 Feb 2022. Accessed 28 Feb 2022.
Centers for Disease Control and Prevention. Investigating Long-Term Effects of Myocarditis. Updated 20 Aug 2021. Accessed 28 Feb 2022.
Centers for Disease Control and Prevention. Interim Clinical Considerations for Use of COVID-19 Vaccines Currently Approved or Authorized in the United States. Updated 22 Feb 2022. Accessed 23 Feb 2022.
Truong, Dongnan T., et al. “Clinically Suspected Myocarditis Temporally Related to COVID-19 Vaccination in Adolescents and Young Adults.” Circulation. 6 Dec 2021.
Patel, Trisha, et al. “Comparison of MIS-C Related Myocarditis, Classic Viral Myocarditis, and COVID-19 Vaccine related Myocarditis in Children.” medRxiv. 07 Oct 2021.
Heymans, Stephane, and Leslie T. Cooper. “Myocarditis after COVID-19 mRNA vaccination: clinical observations and potential mechanisms.” Nature Reviews Cardiology. 09 Dec 2021.
Gargano, Julia W., et al. “Use of mRNA COVID-19 Vaccine After Reports of Myocarditis Among Vaccine Recipients: Update from the Advisory Committee on Immunization Practices – United States, June 2021.” Morbidity and Mortality Weekly Report. 09 Jul 2021.
Oster, Matthew E., et al. “Myocarditis Cases Reported After mRNA-Based COVID-19 Vaccination in the US From December 2020 to August 2021.” JAMA. 25 Jan 2022.
Fox News. ‘The Ingraham Angle’ on COVID restrictions and children. Video. 21 Jan 2022. Updated 25 Jan 2022.
Twitter. Joe Rogan. “If anyone was going to make me look dumb on the podcast I’m glad it’s @joshzepps, because I love him, and he’s awesome. However this is why I was confused: https://theguardian.com/world/2021/sep/10/boys-more-at-risk-from-pfizer-jab-side-effect-than-covid-suggests-study.” 13 Jan 2022.
Singer, Mendel E., et al. “Risk of Myocarditis from COVID-19 Infection in People Under Age 20: A Population-Based Analysis.” MedRxiv. 27 Jul 2021.
Sample, Ian. “Boys more at risk from Pfizer jab side-effect than Covid, suggests study.” The Guardian. 10 Sep 2021. Amended 12 Sep 2021.
Hoeg, Tracy B., et al. “SARS-CoV-2 mRNA Vaccination-Associated Myocarditis in Children Ages 12-17: A Stratified National Database Analysis.” MedRxiv. 08 Sep 2021.
Offit, Paul. Children’s Hospital of Philadelphia. Phone interview with FactCheck.org. 21 Jan 2022.
Wald, Joyce W. Cardiologist, medical director of the shock team and director of heart failure, transplant and mechanical circulatory support program at the University of Pennsylvania Health System. Phone interview with FactCheck.org. 12 Feb 2022.
Elias, Matthew. Cardiologist, Cardiac Center Children’s Hospital of Philadelphia. Phone interview with FactCheck.org. 11 Feb 2022.
Talbot, H. Keipp, and Robert H. Hopkins. “COVID-19 Vaccine Safety Technical (VaST) Work Group.” Powerpoint presentation for Advisory Committee on Immunization Practices. 04 Feb 2022.
FDA. Coronavirus (COVID-19) Update: June 25, 2021. Press release. 25 Jun 2021.
Oster, Matthew. Overview of Myocarditis and Pericarditis. PowerPoint presentation for Advisory Committee on Immunization Practices. 23 Jun 2021.
Wallace, Megan, and Sara Oliver. COVID-19 mRNA vaccines in adolescents and young adults: Benefit-risk discussion. PowerPoint presentation for Advisory Committee on Immunization Practices. 23 Jun 2021.
Oliver, Sara. Evidence to Recommendation Framework: Moderna COVID-19 vaccine, Spikevax. PowerPoint presentation for Advisory Committee on Immunization Practices. 04 Feb 2022.
Oliver, Sara. Summary and Work Group Interpretation: Extended intervals for mRNA COVID-19 vaccines. PowerPoint presentation for Advisory Committee on Immunization Practices. 04 Feb 2022.
FDA. Coronavirus (COVID-19) Update: FDA Takes Key Action by Approving Second COVID-19 Vaccine. Press release. 31 Jan 2022.
FDA. FDA Authorizes Pfizer-BioNTech COVID-19 Vaccine for Emergency Use in Children 5 through 11 Years of Age. Press release. 29 Oct 2021.
FDA. FDA Approves First COVID-19 Vaccine. Press release. 23 Aug 2021.
Vasudeva, Rhythm, et al. “Trends in Acute Myocarditis Related Pediatric Hospitalizations in the United States, 2007–2016.” The American Journal of Cardiology. Volume 149. 15 Jun 2021.
ElAmm, Chantal A., et al. “Characteristics and Outcomes of Patients With Myocarditis Listed for Heart Transplantation.” Circulation: Heart Failure. 7 Dec 2016.
Mevorach, Dror, et al. “Myocarditis after BNT162b2 Vaccination in Israeli Adolescents.” The New England Journal of Medicine. 26 Jan 2022.
Cooper, Leslie T. Department of Cardiology, Mayo Clinic. Email correspondence with FactCheck.org. 2 Feb 2022.
Patone, Martina, et al. “Risks of myocarditis, pericarditis, and cardiac arrhythmias associated with COVID-19 vaccination or SARS-CoV-2 infection.” Nature Medicine. 14 Dec 2021.
Husby, Anders, et al. “SARS-CoV-2 vaccination and myocarditis or myopericarditis: population based cohort study.” The BMJ. 30 Nov 2021.
Buchan, Sarah A., et al. “Epidemiology of myocarditis and pericarditis following mRNA vaccines in Ontario, Canada: by vaccine product, schedule and interval.” MedRxiv. 05 Dec 2021.
Klein, Nicola. Myocarditis Analyses in the Vaccine Safety Datalink: Rapid Cycle Analyses and “Head-to-Head” Product Comparisons. PowerPoint presentation for Advisory Committee on Immunization Practices. 04 Feb 2022.
Moulia, Danielle. Myocarditis and COVID-19 Vaccine Intervals: International Data and Policies. PowerPoint presentation for Advisory Committee on Immunization Practices. 04 Feb 2022.
Tinus, Matthew, et al. Canadian experience and evidence with COVID-19 vaccine primary series extended intervals. PowerPoint presentation for Advisory Committee on Immunization Practices. 04 Feb 2022.
Shimabukuro, Tom. Updates on myocarditis and pericarditis following Moderna COVID-19 vaccination. PowerPoint presentation for Advisory Committee on Immunization Practices. 04 Feb 2022.
Stiles, Steve. “COVID-Vaccine Myocarditis: Rare, Mild, and Usually a Guy Thing.” Medscape. 07 Jan 2022.
Patone, Martina, et al. “Risk of myocarditis following sequential COVID-19 vaccinations by age and sex.” MedRxiv. 25 Dec 2021.
Nuffield Department of Primary Care Health Sciences, University of Oxford. “COVID-19 infection more likely than vaccines to cause rare cardiovascular complications.” 16 Dec 2021.
Daniels, Curt J., et al. “Prevalence of Clinical and Subclinical Myocarditis in Competitive Athletes With Recent SARS-CoV-2 Infection. Results From the Big Ten COVID-19 Cardiac Registry.” JAMA Cardiology. 27 May 2021.
American Academy of Pediatrics. Children and COVID-19: State-Level Data Report. Updated 17 Feb 2022.
Gore, D’Angelo. “Scientist Misleads on COVID-19 Vaccine Effectiveness and Vaccine Safety for Children.” FactCheck.org. 01 Feb 2022.
Spencer, Saranac Hale, et al. “Article Makes Unfounded Claims Linking Athletes’ Injuries, Deaths to Vaccines.” FactCheck.org. 17 Dec 2021.
Calin, Sean. “Soccer Star’s Collapse Was Unrelated to COVID-19 Vaccine.” FactCheck.org. 21 Jun 2021.
Bozkurt, Biykem, et al. “Myocarditis With COVID-19 mRNA Vaccines.” Circulation. 20 Jul 2021.
Liao, George. “Taiwan halts 2nd-dose BioNTech vaccinations for ages 12-17 amid concerns of myocarditis.” Taiwan News. 10 Nov 2021. Updated 30 Nov 2021.
Everington, Keoni. “Taiwan approves 2nd-dose BioNTech vaccinations for ages 12-17, 3rd dose for adults.” Taiwan News. 29 Nov 2021.
“Covid: When can teenagers get a second dose?” BBC. 17 Nov 2021.
Li, Xue, et al. “Myocarditis Following COVID-19 BNT162b2 Vaccination Among Adolescents in Hong Kong.” JAMA Pediatrics. 25 Feb 2022.
Master, Farah. “Hong Kong panel advises single dose of BioNTech COVID shot for teens.” Reuters. 16 Sep 2021.